An anal fistula is a recurrent infection affecting the anus and occasionally the lower rectum. It causes considerable discomfort and disability to sufferers of this chronic condition.
In Singapore, this condition is also known as the 'rat hole' (Laoshudong) amongst the Chinese community and traditional Chinese medical practitioners. It commonly affects economically active adults in the third to fifth decades of life.
Although anal fistulas have been recognized for thousands of years, the treatment of complex or recurrent anal fistulas continues to challenge surgeons today.
A fistula is a medical term describing an abnormal tract with two openings (internal and external) communicating between any two epitheliumlined surfaces.
Therefore, an anal fistula is an abnormal tract communicating between the perianal area to the anal canal and occasionally to the lower rectum.
Anal fistula
How does it arise?
Infection of the anal gland gives rise to anal abscess and unresolved prolonged infection of these anal glands results in the formation of anal fistula (cryptoglandular hypothesis).
90% of all anal abscesses result from non-specific infection of the anal glands. We do not know why certain individuals are prone to this infection but approximately 25% to 30% of these patients with anal abscesses will eventually end up with an anal fistula1.
Only people with susceptible anal glands can develop an anal abscess and eventually an anal fistula.
Natural History of the Anal Fistula
Anal fistulas and anal abscesses are separate phases along the spectrum of a common infective condition affecting the anus. The abscess represents the acute stage whereas the fistula is the representative of the chronic phase.
The anal canal is a muscular tube approximately 3–4 cm long, connecting the rectum to the anal verge. It is made up of two cylindrical muscle tubes called the outer and inner anal sphincter muscles. Anal glands are found in between these two muscle tubes at the level of the dentate line (approximately 2cm from the anal verge).
Anal Abscess Fig. 1
Anal Abscess Fig. 2
The role of these anal glands in human is unknown. it is believed that the duct from the anal glands becomes blocked, resulting in stasis, infection and subsequent abscess formation. Persistent infection of the anal gland and its duct results in the formation of anal fistula.
The 'Simple' and the 'Complex' Anal Fistula
As the duct from the infected anal gland leading into the anal canal is blocked, the accumulated pus may spread in other directions. It usually follows the path of least resistance. The path created will determine the type of anal fistula formed.
An anal fistula usually has two openings — an internal opening in the anal canal and an external opening outside the anal verge.
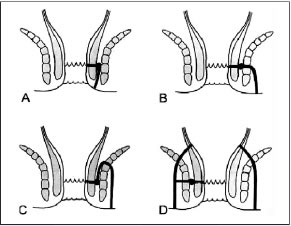
A simple standard classification of the types of anal fistula was described by Parks et al2 (as shown on the next page). This classification is particularly helpful in determining the type of treatment required by the patient.
There are basically two broad groups of anal fistula in clinical practice — simple and complex anal fistula.
The 'complexity' of the anal fistula is basically dependent on:
The amount of anal sphincter muscle involvement
The presence of more than one anal fistula (secondary tract) and/or with abscess cavity
Anal fistula with tracts above the anal sphincter complex or with the internal opening in the lower rectum or with the external opening further away from the anal verge
Anal fistula associated with other diseases (e.g. Crohn's disease, tuberculosis)
A. Inter-sphincteric Anal Fistula B. Transphincteric Anal Fistula C. Supra-sphincteric Anal Fistula D. Extra-sphincteric Anal Fistula
'Complex' is a more severe form of anal fistula and will definitely require more complicated treatment. Surgical treatment for these fistula is sometimes carried out in stages.
Fortunately, the majority of anal fistulas are of the 'simple' type and therefore easily treatable with positive outcomes and low recurrence rates.
Such simple types of fistulas usually:
Are of the low intersphincteric or transphincteric type
Single short tract
Have an external opening that is close to the anal verge
Have an internal opening that is lower (closer to the anal verge)
Are absent of any secondary tract or abscess cavity
Are absent of any association with other diseases
Any other anal fistulas that do not fulfil the criteria stated above are considered 'complex'. Fistulas that persist or recur despite treatment are also considered to be 'complex' as they are difficult to treat.
How do Patients with Anal Fistula Present?
As stated earlier, anal fistulas and anal abscesses are two different phases in the spectrum of a common infective condition affecting the anus. Therefore, a patient with an anal fistula will often recount a history of an anal abscess that has been drained either surgically or spontaneously.
Usually, patient complained of intermittent anal pain and anal swelling followed by discharge and resolution of these symptoms. There is occasional low grade fever during these episodes. Patients may also notice a small lump in the perianal region with occasional bleeding associated with defecation.
Additional bowel symptoms may be present when the anal fistula is associated with other conditions (e.g. proctocolitis, Crohn's disease, cancer, tuberculosis or actinomycosis).
How to Examine and investigate an anal fistula
How fistulas are examined?
The external opening may be seen as an elevation of granulation tissue discharging purulent liquid. However the internal opening may not be apparent The number of the external openings and their location may be helpful in locating the internal opening and subsequently classifying the type of anal fistula present in the patient.
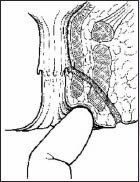
Digital examination of Fistula
As a rule of thumb, the greater the distance of the external opening from the anal margin, the greater the probability of a complicated extension.
Clinical examination may reveal an indurated cord-like structure underneath the skin in the direction of the internal opening with asymmetry between right and left sides. It is important to note for perianal surgical scar from previous fistula surgery to detect fistula relapse or recurrence. This will then alert the clinician of a possibility of a complex fistula which may require specialist care. Bidigital rectal examination must be performed to define the relationship of the tract with the anal sphincter muscles. It also provides information regarding pre-operative anal sphincter tone at rest and on squeezing because of the risk of faecal incontinence.
How fistulas are Investigated?
Investigations to be performed in patients with anal fistula is divided into two categories:
Diagnosis and classification of anal fistula
Assessment of integrity and function of anal sphincters
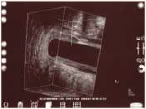
Anoscopy must be performed to identify the internal opening. Sigmoidoscopy should be performed to locate the internal opening and to exclude underlying secondary pathology. Occasionally, total examination of the large bowel is required either using colonoscopy or barium enema in patients with atypical, complex, multiple or recurrent anal fistula who have symptoms suggestive of inflammatory bowel disease. Endoanal ultrasonography is useful in the total assessment of anal fistula. It allows imaging of the fistula tract to provide information on the complexity of the anal fistula, detect the presence of secondary abscess cavity and establish relationship of the fistula to the anal sphincter complex.
Endoanal Ultrasound Fig. 1
Endoananl Ultrasound Fig. 2
Other modalities such as fistulography and magnetic resonance imaging are available to further delineate 'difficult' and complex recurrent anal fistula. Pre-operative assessment of the anal sphincter function is not generally required. However, it may be useful as an adjunct to planning operative approach in patients with recurrent fistula, women with previous obstetric trauma and elderly patients. Resting and squeezing anal pressure can be measured preoperative to aid in the discussion and planning of the management of 'difficult' anal fistula.
Principles of Management
The general principles of fistula management are to:
Eliminate the fistula
Prevent recurrence
Preserve anal sphincter function
Surgery
Surgery is the mainstay of management of anal fistula. The role of medical management is mainly in the usage of antibiotics to treat recurrent low grade infection associated with the anal fistula especially in patients with immunocompromised medical conditions (e.g. diabetes mellitus).
There are several surgical methods used in the eradication of the fistula tract and the option depends on the type of fistula tract present.
Lay-Open Technique - This is the most common procedure for simple anal fistula (low intersphincteric or transphincteric fistula). The tract is incised to deroof it to allow adequate drainage for secondary healing to take place.
Lay Open Technique
Seton - A seton is a foreign material inserted into a fistula tract to encircle the anal sphincter muscles. It is used to treat high anal fistula whereby simple lay-open method might render the patient incontinent.
Fistulectomy - The fistula tract is totally excised upto the anal sphincter muscle complex leaving the wound for secondary healing.
Seton Insertion
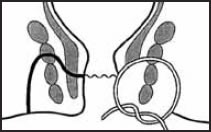
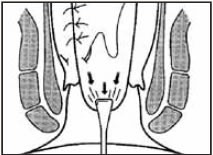
Anorectal Advancement Flap - This is a more complicated technique used when the conservative laying-open method is not appropriate eg. in anterior fistulas in women, high complex fistulas and previous multiple anal sphincter surgeries. The internal opening is excised and then closed with a full-thickness flap of rectal mucosa.
Anorectal Advancement Flap
Fibrin Glue - This is a non-invasive approach whereby the fistula tract is closed using fibrin glue.
Bioprosthetic Fistula Plug - This is a relatively new technique using a bioprosthetic plug to close the fistula tract. However, results are equivocal and cost are high.
Post Operative Care
After surgery, patients are advised to take a high fibre diet with plenty of fluid. They are prescribed stool bulking agents, stool softener and analgesia. Patients are instructed to take frequent sitz baths to ensure perianal hygiene. Daily wound dressing at nearby clinics are usually required in the first week after surgery.
(Sitz bath - Please refer to previous Colorectal Clinic S-files Volume 1 Issue 2 Dec 2006)
'Difficult' Fistula and Recurrent Fistula
These fistulas are best managed by specialists to ensure the best possible outcome. The risk of complications arising from the management is high. It is prudent to ensure thorough pre operative assessment to delineate all the tracts and cavities, study the anal sphincter bulk and function to plan the most ideal surgical option.
Prevention
As mentioned earlier, the formation of the anal fistula is totally unpredictable. The only way to prevent the disease is to reduce the incidence of infection of the anal glands which is the precursor of anal fistula. Good perianal hygiene is an important step to prevent this uncomfortable condtion.
Anal Fistula in a nutshell
An anal fistula is a chronic infection of the anal glands in the anal canal.
The majority of the anal fistula are the 'simple type' and easy to treat.
Anal fistula must be assessed thoroughly by a surgeon to plan the most optimal management to prevent recurrence and reduce risk of complication.
Recurrent anal fistula should be evaluated by an experienced Colorectal Surgeon with adjunct investigations (e.g. anal manometry and endoanal ultrasonography) before deciding on the appropriate therapy.