The NUH Hernia Centre is the first dedicated centre in Singapore offering comprehensive hernia repair procedures. The centre was established to address the growing need for specialised care to tend to the increasing number and diversity of individuals affected by hernia-related conditions. Annually, we see over 400 new hernia cases, with a yearly rise of 10 - 15%.
Our multidisciplinary group of hernia specialists use a variety of surgical techniques and are among the first in the world to apply robotic-assisted surgery in complex abdominal wall hernia and reconstruction.
What is a hernia?
A hernia is a bulge over the abdominal wall caused by a weakness or tear of the muscles, leading to the protrusion of organs like the intestines and abdominal fatty tissue through the weakened area. Patients usually notice a swelling under the skin and may occasionally experience pain and discomfort. Symptoms may worsen after prolonged standing, walking or strain, such as lifting heavy objects.
What are the different types of hernias?
Hernias are named according to their location on the abdominal wall or their specific cause.
Groin Hernia: There are two types of groin hernias – Inguinal and Femoral. Inguinal hernia is the most common type of hernia and has two varieties – Indirect and Direct. Indirect hernia occurs through the groin in an area on the muscle where the male testis pierces and descends down during foetal development. Femoral hernia is more common in women and is known to cause acute problems.
Umbilical Hernia: This is one of the most common hernias. Women are more commonly affected than men – likely due to a previous pregnancy. This area is particularly weak because of the umbilical cord attachment during birth.
Incisional Hernia: This form of hernia develops at the site of previous surgical incisions. The muscles around the incision site become weak and this may lead to hernia formation. Multiple areas of weakness may develop with multiple hernias along the entire length of the scar. These hernias can develop weeks, months or years after the initial surgery. Every subsequent surgery further weakens the muscle and increases the risk of hernia formation.
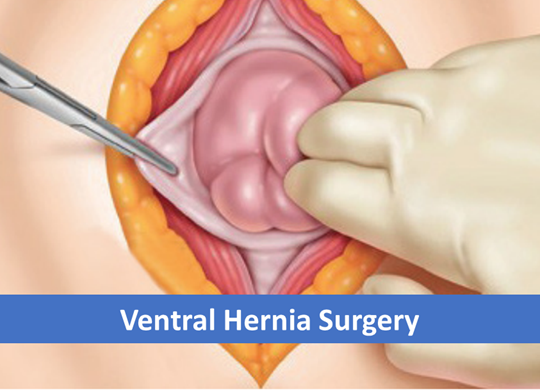
Midline Ventral Hernia: This can be epigastric (in upper abdomen), para-umbilical (around the umbilicus), supra-pubic (in lower abdomen) and sub-xiphoid (just below the rib cage in the midline).
Spigelian Hernia: This occurs through the spigelian fascia which is just beside the rectus muscles of the abdomen. The hernia lies in between two muscles of the abdominal wall and is hence difficult to diagnose clinically. The surgeon may need to perform an ultrasound or computed tomography (CT) scan.
Rare Hernia: This includes lateral hernia, obturator hernia, lumbar hernia, sub-xiphoid hernia and parastomal hernia.
Most hernias occur as a result of weakness or defect in the muscles of the abdomen since birth. As one ages, this defect is further weakened by strenuous physical activity, lifting of heavy objects or incisions of a previous surgery. The risk of developing a hernia increases with:
Straining due to constipation or when passing urine
Smoking
Obesity
Taking medications
In most instances, a hernia can be diagnosed through a physical examination. However, in cases of recurrent hernias, complexity or within specific patient groups (such as obese or those with prior surgeries), an imaging diagnosis (ultrasound, CT scan or MRI) may be required. Surgical repair is often necessary for most hernias to alleviate symptoms and prevent complications, such as intestinal strangulation. Trusses or abdominal binders serve as temporary measures for patients awaiting surgery or those at high risk.
In addition to Open and Laparoscopic (Keyhole) Surgery, we perform novel surgical techniques, including Single Incision Laparoscopic (SILS) Hernia Repair, Robotic Surgery, as well as Muscle Release surgeries such as Endoscopic Component Separation and Transversus Abdominis Release.
Following a comprehensive examination, your surgeon will determine the most suitable treatment options for your specific case.
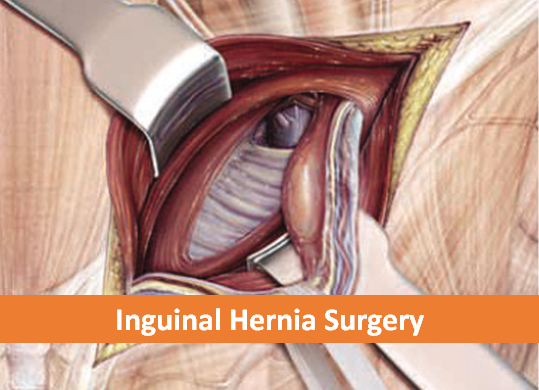
Inguinal Hernia Surgery
Open Hernia Repair Laparoscopic (Keyhole) Surgery - TAPP (Transabdominal pre-peritoneal) - TEP (Totally extra-peritoneal)
Robotic Surgery Surgery involving large incisions can often result in increased pain and wound complications. Robotic surgery is an advanced technology allowing surgeons to perform complex manoeuvres not possible through laparoscopy. This technology enables surgeons to conduct procedures through similar small incisions, reducing the impact of larger cuts.
Single Incision Laparoscopic (SILS) Hernia Repair This surgical approach involves just one incision, typically around 1.5-2 cm in the abdominal region. Using a single incision tends to result in reduced pain and improved cosmetic outcomes.
Endoscopic Component Separation (ECS)
In hernias with large defects, closure of the abdominal wall can be challenging. The surgeon may incise the muscles in the lateral abdominal wall to release attachments and bring them towards the midline to cover the defect.
What should you expect after a day surgery procedure?
Following the surgery, you will be transferred to the recovery until you are fully awake. You will be discharged once you are awake and able to pass urine and walk . Upon your discharge, you will be seen at the clinic. As with any hernia surgery, you may experience some soreness, mostly during the first week post-surgery. With Laparoscopic Hernia Repair, you will be able to resume your normal activities within a shorter time. Avoid activities that require straining (such as weight-lifting) for at least the first 2 weeks post-surgery.
What are the complications that can occur?
All surgeries carry potential complications, including:
Bleeding and infection
Difficulty urinating after surgery is not common. However, a temporary tube may be inserted into the urinary bladder.
Collection of fluid at the site of the hernia (seroma) may happen in large hernia; in most cases, the fluid will be reabsorbed within 4-6 weeks post surgery, an rarely requires an intervention.
Minimal risks include injury to the urinary bladder, intestines, blood vessels, nerves or the sperm tube going to the testicles that may require a conversion to open surgery or a reoperation.
Late complications are possible recurrence of the hernia and chronic pain.
When should you call your doctor?
Contact your physician or surgeon if you experience any of the following:
Persistent fever above 38.5 degrees Celsius
Bleeding
Increasing abdominal pain
Pain that is not relieved by medications
Persistent nausea or vomitting
Inablitiy to urinate
Chills
Persistent cough or shortness of breath
Purulent drainage (pus) from any incision
Redness surrounding any of the incisions that is worseninig or getting bigger
Sub-specialties: Bariatric & Metabolic Surgery, Chronic Programme (Live Better), FAST Programme (Get Better), General Surgery, Minimally Invasive Surgery, Upper Gastrointestinal Surgery Special interests: Abdominal Wall Pathophysiology and Hernia Surgery, Obesity and Metabolic Syndrome, Research in Robotics, Surgical Devices, Simulators and Education
Sub-specialties: Chronic Programme (Live Better), FAST Programme (Get Better), General Surgery, Trauma Surgery Special interests: Trauma Surgery, Critical care, Minimally-invasive Surgery (Acute care surgery)
Sub-specialties: General Surgery, Minimally Invasive Surgery Special Interests: Minimally Invasive Surgery, Complex Hernia Surgery, Diagnostic and Therapeutic Endoscopy
Many patients notice a visible bulge in the abdominal area. Some experience pain at the bulge, particularly during strain or physical activity. Typically, hernias are diagnosed through routine clinical examinations. In specific cases, an ultrasound or CT scan may be recommended, especially for larger or recurrent hernias or in patients with complexities, such as obesity.
Why do patients need surgery?
Most hernias need to be repaired surgically to treat symptoms and prevent complications (e.g., strangulation of intestine). Truss or abdomindal binder are just temporary measures while awaiting surgery.
What happens if patients do not undergo surgery?
The only treatment for hernia is surgery to repair the defect in the muscle. By not undergoing surgery, the hernia may increase in size and a portion of the intestine or fat inside the abdomen may pass through the defect and get trapped. This may lead to blockage or strangulation of the intestine. Patients may also get a sudden onset of abdominal pain, distention of abdomen, persistent vomiting and constipation.
What is the type of anaesthesia used?
At NUH, most hernias are operated under General Anaesthesia (GA). Local Anaesthesia (LA) can also be an option for patients who are not suitable for GA.
What is the length of stay in the hospital?
Most patients return home on the same day. A small number of patients may stay overnight for various reasons, such as pain. Patients with large or complex hernia may have to be warded for a few days, depending on the complexity of the surgery.
What are the advantages of Laparosopic Hernia Repair?
Results may vary depending on the type of procedure and each patient’s overall condition.
Advantages of this procedure:
Less post-operative pain
Shorter hospital stay
Faster return to regular diet
Faster return to normal activity
Improved physical appearance
What do I need to prepare before a Hernia Surgery?
Depending on your age and medical conditions, pre-operative preparations include:
Blood tests
Chest X-rays
Electrocardiogram (ECG)
You are also advised to adhere to the following:
Shower the night before or morning of the operation
Fast the night before the operation from 12am, but continue to take the medications that are permitted by your surgeon.
Drugs such as aspirin, blood thinners, anti-inflammatory medications (arthritis mediciations) and Vitamin E may need to be stopped temporarily for a week, prior to surgery.
Quit smoking
Arrange for any help you nay need at home post-surgery
The NUH Hernia Centre prioritises ongoing research to elevate clinical service standards. Our contributions in hernia research have led to innovative approaches that enhance holistic patient care and improve post-surgery quality of life.








_v2.jpg?sfvrsn=2b4d6ed7_1)

/usc.png)